Our Bones Tell The Story | The Screw-Home Mechanism
The surface of our joints tells the story of how they are designed to move and the potential movement that’s available to us. We know that our knee bends and straightens, but often forget it also has the ability to rotate. Rotation does in fact occur at the knee, and is greatly affected by both our feet and our hips; as the knee straightens (extends), the hip and knee are both externally rotating but the hip rotates faster which creates a relative internal rotation at the knee.
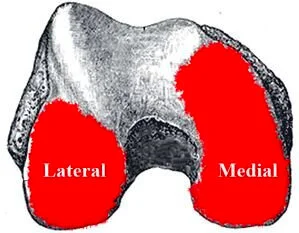
A view of the distal end of the femur showing the unequal amount of joint surface available for movement internally and externally.
The femur has two rounded ends (condyles) and one side has more surface area than the other, allowing more movement internally (medially) than externally (laterally). After the lateral condyle has moved to full range there is still surface area for the medial condyle to move into and this is the known as the ‘screw-home’ mechanism.
The ‘screw-home’ mechanism is the rotation between the tibia and femur and is considered to be a key element to knee stability for standing upright. This mechanism serves as a critical function of the knee and it only occurs at the end of knee extension, between full extension (0°) and 20° degrees of knee flexion.
As the knee approaches terminal extension it is in its most stable position; the tibia is in the position of maximal stability with respect to the femur and the leg is able to support the body weight despite the quads not being activated. The anterior cruciate ligaments (ACL) plays an important role in the process and any ACL problems may restrict or stop the screw-home mechanism.

Credit: Dr. Bhupendra Gosai
The screw-home mechanism reverses during knee flexion and when the knee begins to flex from a position of full extension, the hip internally rotates faster than the knee, this creates a relative external rotation at the knee.
Our symptoms may be at the knee, but we need to retrace the origins of dysfunction and improve mobility and joint-Loading capacity elsewhere
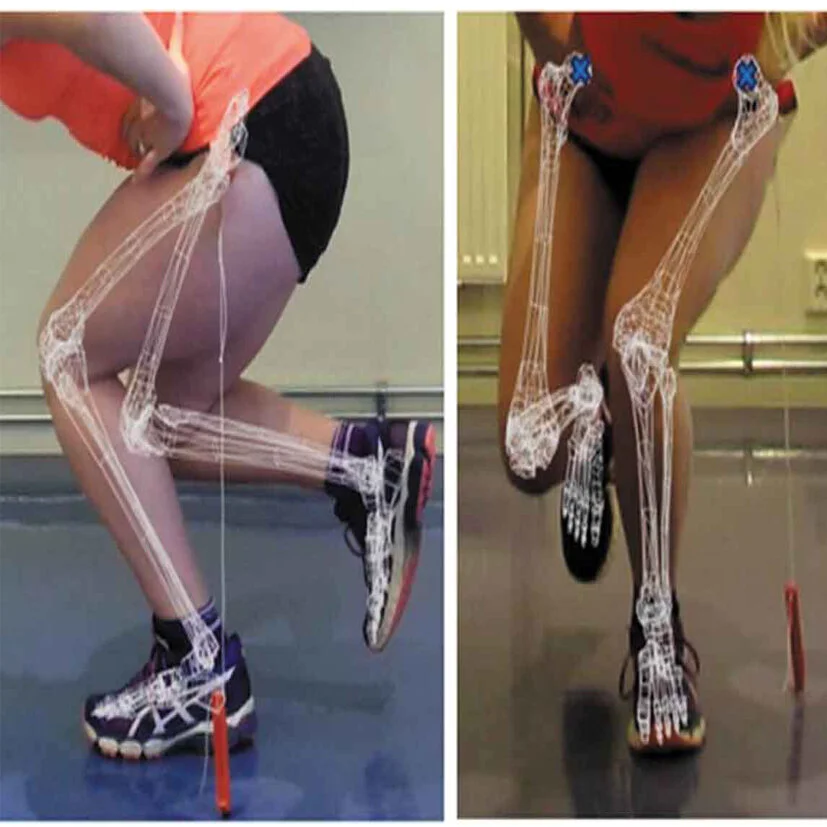
A supinated foot couples with an internally rotating hip and externally rotating tibia and the opposite occrurs in a pronated foot; an externally rotating hip couples with an internally rotating tibia. If any of these joint motions are not fully accessible or sequenced, it could potentially lead to excessive motion at the other joints, increasing mechanical stress and creating compensations and adaptions that lead to problems.

There are numerous potential ways in which any one person can compensate around dysfunction. Josh Landis describes two scenarios which can show up as knee pain:
An immobile navicular bone in the foot is preventing full pronation in the foot. A lack of adequate pronation then leads to increased subtalar inversion, which shifts the talus position medially. The talus shifting medially then neurologically inhibits all the muscles in the lower extremity moving laterally. Decreased muscle strength of the glute medius, TFL, and other abductors then destabilizes the hip leading to an aggressive knee valgus, and the medial knee becomes painful.
An unstable SI joint stuck in anterior torsion. This decreases the hip joint’s available external rotation. A lack of hip external rotation then becomes compensated for by increased external rotation of the tibia. Excessive external rotation of the tibia then leads to an imbalance between the lateral and medial hamstrings over time. The lateral hamstrings have more mechanical stress on them, and over time we start to get pain in the posterior lateral knee.
if the knee cannot fully extend the screw-Home mechanism can’t happen
In order to fully understand and resolve our knee symptoms, we need to consider rotational stability as well as take into account how things are functioning above and below at the hip and foot. Once we have this information, then it’s possible to integrate and couple movements at the foot, knee and hip. If you’re unable to fully straighten your legs then your quadriceps are always activated and this means that your body has to rely on muscles and ligaments for support and stability, leading to over-work, pain and increased risk of injury.
- F
REFERENCES
Hallén, L. & Lindahl, O (2009). The “Screw-Home” Movement in the Knee-Joint. Acta Orthopaedica. 37. 10.3109/17453676608989407
Laubenthal KN. A quantitative analysis of knee motion during activities of daily living. Phys Ther 52(1):34-43;1972
Rowe PJ et al. Knee joint kinematics in gait and other functional activities measured using flexible electrogoniometry: how much knee motion is sufficient for normal daily life? Gait and Posture 12:143-155;2000



























What are the most common misconceptions about furniture free? Well these are my top three!